Update (2021-12-13): This post is wrong in several places:
In Australia, the AstraZeneca vaccines were not recommended for younger people (by TGA? ATAGI? I don’t remember), so I wound up getting the Pfizer vaccine.
I was under the mistaken impression that AstraZeneca was a “traditional” vaccine made from inactivated SARS-CoV-2 virus. It isn’t: it is an adenovirus that infects but does not replicate within human cells, and it instructs infected cells to produce SARS-CoV-2 spike protein.
Despite assurances from the Prime Minister that the vaccine will not be mandatory, everyone is falling over themselves to implement mandates.
We didn’t get to go back to normal life, because the vaccines turned out to offer temporary, non-sterilising protection, and variants keep popping up.
TL;DR: Despite earlier reservations, I will probably be taking a vaccine when offered, but it would be for different reasons if I was outside Australia. Also, continue to watch out for manipulation and fudging from authorities.
(Note: Twitter links have screenshots next to them, as it’s notoriously difficult to predict what Twitter shows on the other end of a link.)
Emergency approvals for the major vaccine candidates (Pfizer/BioNTech, Moderna, Oxford/AstraZeneca) have been issued, and it’s time to scale up and deploy. Then we reach herd immunity and get back to normal life, right? Well, first we need to make sure we’re all talking about the same “herd immunity”, and watch closely for shifting definitions. Between November and December 2020, the WHO’s website changed its definition of “herd immunity” at least twice (emphasis in the quotes is mine):
Herd immunity is the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection.
‘Herd immunity’, also known as ‘population immunity’, is a concept used for vaccination, in which a population can be protected from a certain virus if a threshold of vaccination is reached.
‘Herd immunity’, also known as ‘population immunity’, is the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection. WHO supports achieving ‘herd immunity’ through vaccination, not by allowing a disease to spread through any segment of the population, as this would result in unnecessary cases and deaths.
The 2020-11-24 definition attempts to enforce the consequent — the actual goal is to reach herd immunity through vaccination instead of exposure. Instead of just saying that, the WHO instead claimed that “herd immunity” requires vaccination. I suspect the 2020-11-31 change only happened because people noticed and kicked up a stink, and this is why it’s always important that we keep paying close attention and hold institutions to account. They’ll take lazy shortcuts otherwise.
What else is changing? Well, we have Dr. Fauci shifting the herd immunity goalposts (emphasis in quotes mine):
In a telephone interview the next day, Dr. Fauci acknowledged that he had slowly but deliberately been moving the goal posts. He is doing so, he said, partly based on new science, and partly on his gut feeling that the country is finally ready to hear what he really thinks.
[…]
Dr. Fauci said that weeks ago, he had hesitated to publicly raise his estimate because many Americans seemed hesitant about vaccines…
[…]
“When polls said only about half of all Americans would take a vaccine, I was saying herd immunity would take 70 to 75 percent,” Dr. Fauci said. “Then, when newer surveys said 60 percent or more would take it, I thought, ‘I can nudge this up a bit,’ so I went to 80, 85.”
It is despicable to gripe that people aren’t “trusting the science” and then admit that you’re making decisions based on gut feelings. The new mutations from UK and South Africa are more transmissible and are spreading almost world-wide. This will increase the herd immunity threshold (which is 1 − 1/R, so if R increases, so does the threshold). But this manipulation is disgusting. It’s no wonder people are hesitant about the vaccines when they can see the manipulation taking place at other levels (remember “masks don’t work”? I do).
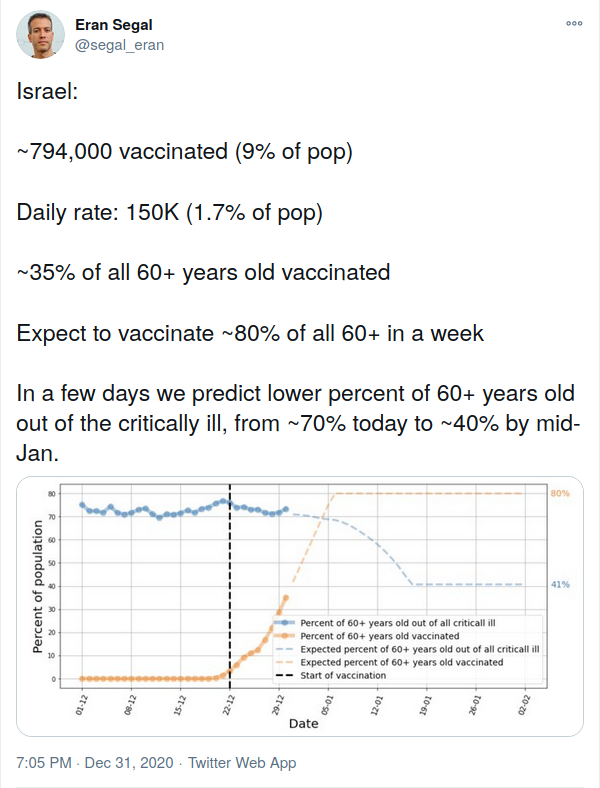
We now need more people than ever to get jabbed, and the faster the better. We have the emergency approvals, so all we need to do is crank up production, get doses into people’s arms and this is over? Right? I mean, that’s what Israel’s doing (screenshot): vaccinating 24 hours a day, 7 days a week, including Shabbat. This is what actually trying looks like.
How about the rest of the world? Here’s a vaccine rollout tracker. Zvi has another giant post about this week in COVID. The stuff about rollouts starts at “All I Want For Christmas is a Covid Vaccine, But They Somehow Underpriced Them So Much No One’s Even Bothering To Sell Out”, and nobody is actually trying:
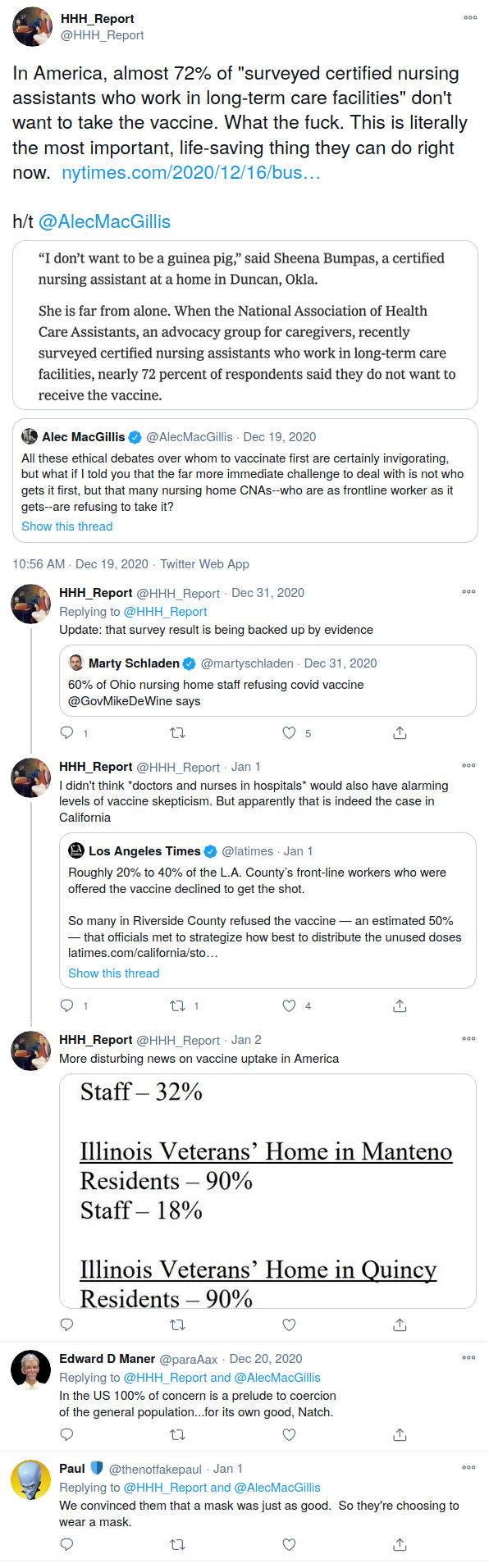
It doesn’t matter how bad the rollout machinery is if nobody is taking the doses. It doesn’t look good so far (links go to twitter threads):
Would I take a vaccine? I’ve been hesitant about the SARS-CoV-2 vaccines (the mRNA ones in particular), and I know I’m not alone among my friends. Not because we’re anti-vaxxers, but because the vaccine approvals seem somehow too fast and too slow: the trials don’t feel long enough, but when it was time for the FDA to actually issue an emergency approval, they took Thanksgiving off and scheduled a meeting to look over Pfizer’s data three weeks after submission (NB: the comment section is probably better than the article).
So why have I changed my mind? I’m concerned by these “musings of an anonymous, pissed-off virologist” (repeated below because screenshots of text suck):
As viruses go, SARS-CoV-2, is quite easy to neutralize with antibodies and, it turns out, straightforward to generate effective vaccines based on the spike protein. Perhaps, even probably, those two properties are causally related. Moreover, it appears that it is quite hard (albeit not impossible) to generate resistant spike variants that evade the polyclonal antibody responses elicited by said vaccines. This is all excellent news.
However, if I had a nefarious nature and wanted to ensure that the new SARS-CoV-2 vaccines were rendered impotent, these are a few things I would try.
First, we’d want to maximize the viral population size and diversity. Because SARS-CoV-2 has a proof-reading polymerase, we might have to work hard to do this. The four measures outlined below might help accomplish this, assisting the virus to explore as much genetic diversity as possible, generating every conceivable point mutation as frequently as possible.
- Delay the rollout of testing, so that the virus could spread undetected, seeding outbreaks in geographically, demographically and culturally diverse host populations, rendering it virtually impossible to quash with test-trace-isolate approaches.
- Implement partial and patchy restrictions on movement and social interactions, thus maintaining consistently large pools of infected individuals.
- Keep schools open, claiming that children don’t frequently transmit SARS-CoV-2. Because children have generally mild and perhaps more frequently asymptomatic infections, diversifying viral populations are more likely to spread undetected.
- Start a rumor-mill, making full use of social media and other outlets, with topics such as masks are unnecessary or don’t work, that PCR tests are too sensitive or unreliable, that infection-induced ‘herd immunity’ is a reasonable strategy, or even that SARS-CoV-2 isn’t real. Undermining already inadequate public health measures helps keep viral population sizes large.
Second, during or after the establishment of large and diverse viral populations, we’d begin to apply selection pressure to enrich antibody resistance mutations. For that, we would elicit the help of the medical establishment to implement measures 5 and 6. They, laudably, want to help as many people as possible as quickly as possible — we could exploit this.
- Treat tens of thousands of people with uncharacterized convalescent plasma of weak/unknown potency, without proper clinical trials, to get the ball rolling in applying some selection pressure to enrich for antibody resistant variants. (Again, I don’t know how effective this would be since it is mostly done in hospitals, where onward transmission would presumably be rare, but it would certainly be worth a try) Immunocompromised individuals with persistent infection might be especially helpful here.
- Finally, and here’s the kicker: having developed a remarkable two-dose vaccine, that is extraordinarily effective, ADMINISTER IT TO MILLIONS OF PEOPLE — BUT DELAY THE SECOND DOSE. Generating a pool of hosts with just the right amount of neutralizing antibody to apply selection pressure, but also maintain sufficient levels of partially antibody-resistant virus to allow onward transmission is key here. We might not achieve this shortly after the first dose, but if we let immunity wane for a little while, say 4 to 12 weeks, we just might hit the sweet spot. Of course, I don’t know if the above would be successful, but that’s what l’d try if I wanted to generate vaccine-resistant SARS-CoV-2 variants.
The world’s pathologically (heh) bad response creates a rich environment for mutations (e.g., the new UK strain, similar mutations in South Africa) and potential for vaccine escape. If I was living overseas, I would seriously consider taking any of the offered vaccines, for the following reasons:
The risk trade-off is much higher because there’s a lot more virus going around. Containment of the UK strain has failed, and it’s been detected in the US and all over Europe.
Faster vaccination rollout limits the amount of time the virus has to mutate and get around vaccine-derived antibodies.
The current degree of lockdown is extremely unpleasant, compliance is waning, and the lockdown required to contain the new strain is unthinkable (and probably unachievable).
However, I have seen a couple of things that make me a bit cautious. I mention them for completeness but still think getting the jab (when offered) is correct overall:
Obviously and badly stage-managed vaccinations. I can’t find the links, but I remember seeing VIPs getting jabbed with empty or spring-loaded syringes, and a nurse who fainted after receiving the vaccine. She later claimed to be “prone to fainting spells” — why would you put someone like that in front of the cameras?
Four participants in the vaccine group of one of the Pfizer trials developed Bell’s Palsy (page 6), compared to zero in the placebo group. Even so, this is lower than the incidence of Bell’s Palsy in the general population.
But in Australia, we’re not expecting to see rollout until March or so, and so my thoughts are a bit different. Here, I would probably take the Oxford/AstraZeneca vaccine, if offered. By the time any mRNA vaccines are offered, we should know from the overseas rollout whether there’s anything to watch out for. Here are my reasons why I’m okay with that rollout timeline, and willing to stay a bit cautious around the mRNA vaccines:
We don’t have widespread community transmission because our hotel quarantine (mostly) works.
Note: This is not a one-sided trade-off. As demonstrated by the 2020-21 outbreak, our quarantine system is brittle, and nobody wants a repeat of what Melbourne went through. If we had widespread vaccination, we wouldn’t be creating so much waste (e.g., discarded masks), and domestic tourism would be much more stable. The mismanaged outbreak in Sydney killed regional tourism over NYE, which was a brutal follow-up for those places hit by the 2019-20 bushfires.
We probably won’t start seeing the vaccine rollout for a couple of months. This means we get to watch the world for more safety data (particularly for the mRNA vaccines, which are being deployed for the first time against COVID-19).
Australians are more likely to be vaccinated using the Oxford/AstraZeneca vaccine than an mRNA vaccine. We have domestic manufacturing capacity (CSL will manufacture 30M of the 33.8M Oxford/AstraZeneca doses on order, but we can’t make mRNA vaccines), it’s cheaper per dose ($6-7 vs $40-60 per person for the mRNA vaccines), has less strict cold chain requirements (Pfizer needs storage at -70°C, Moderna at -20°C for long-term storage), and is based on proven techniques (an altered virus that doesn’t grow inside human cells).
It is not being made mandatory.
“We will be making the vaccine free and voluntary,” Mr Morrison said.
After a year of noble lies and deceitful manipulation of the public, this says that the vaccine can stand on its own merits, and that’s a massive breath of fresh air.
We are not at the end, we haven’t yet seen the light at the end of the tunnel, but we should soon see the first pinprick of that light. It’s time to close this out.
{kind=link}
{kind=link}
{kind=link}